




Transcatheter aortic valve implantation (TAVI)
What is Aortic Stenosis (AS)
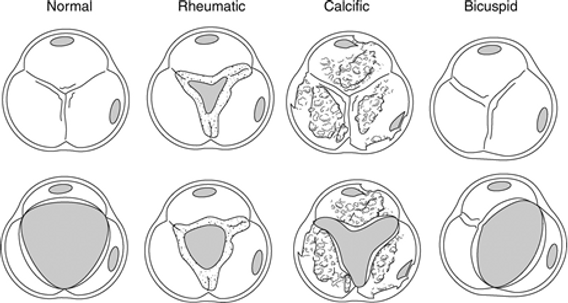
Aortic Stenosis (AS) refers to the pathological thickening of the aortic valve and the fusion of the leaflets of the aortic valve, resulting in reduced mobility and functionality of the aortic valve. Causes of AS include calcific AS, congenital AS or rheumatic AS. With the current ageing population, calcific AS is the most common cause and tends to degenerate further with age. Patients with severe AS often present with chest pain, shortness of breath on exertion or even syncope. Once the symptoms begin to occur in patients with severe AS, the prognosis is bleak, as the average survival rate is less than 2-3 years.
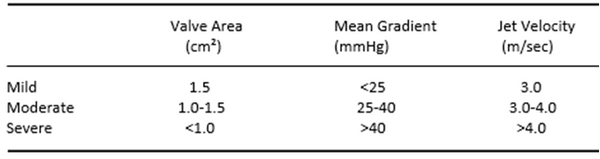
Currently the severity of AS is determined by the mean pressure gradient across the aortic valve (left ventricular pressure and aortic pressure), the size of the valve area and the jet velocity across the valve. As AS progresses, the resistance of blood flow increases, resulting in an increased peak-peak and mean gradient across the aortic valve and a slurred upstroke of the aortic pressure due to the delayed opening of the aortic valve. Moreover, the size of the valve area decreases with disease progression.
AS severity
Treating AS
The most successful treatment for patients with severe AS is aortic valve replacement.
-Those with multiple comorbidities may be considered too high risk for surgical AV replacement, but may qualify for TAVI.
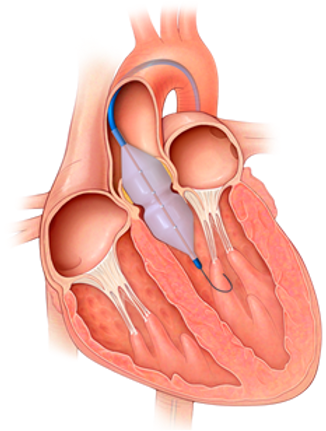
Balloon aortic valvuloplasties are performed by inflating a balloon across the aortic valve to dilate the stenotic aortic valve and decrease the gradient across the aortic valve. Balloon aortic valvuloplasties only provide successful short-term outcomes and are typically performed for palliation or to possibly improve suitability for other procedures such as transcatheter aortic valve implantation.
Procedure
Procedure
-
Typically done through groin access - both sides accessed.
-
Venous access for temp pacing wire into RV
-
Arterial access x2, 1 for delivery system and 1 for gradient measures
-
RV temp pacing wire inserted into RV and pacing settings tested
-
Catheter into Ao
-
Catheter crossed into LV across AoV (usually with a wire)
-
Baseline pressures collected
-
Pre valve balloon may be utilised (BAV- balloon aortic valvuloplasty)
-
TAVI deployed
-
Post valve insertion ballon may be utilised
-
Rapid pacing is usued during BAV and valve deployment to limit flow across AV to allow for accurate positioning.
-
Post deployment gradients are calculated
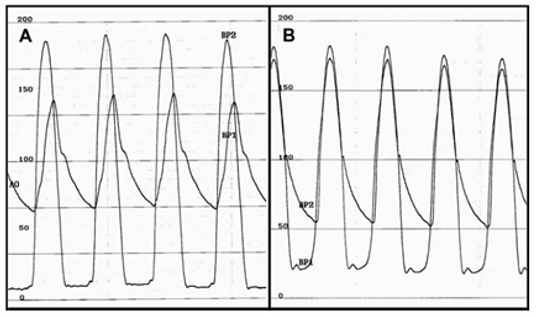
Pre and post gradient measurements
Balloon inflation across the aortic valve
Pressure drop associated with rapid ventricular pacing during balloon inflation
