




Wide awake
-decoding broad complex tachycardias-
Patient presentation
-
29 year old female
-
history of slow pathway ablation for typical AVNRT
-
Recurrent palpitations
-
reported wide complex tachycardia by ambulance (not documented)
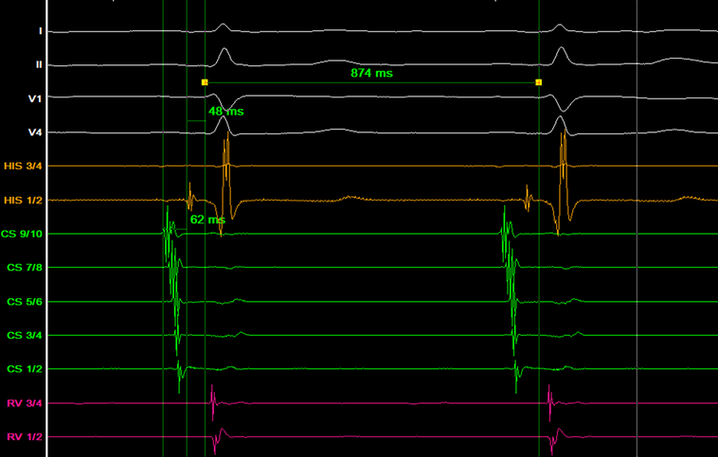
Baseline ECG

Baseline ECG/EGM
-
AH: 62
-
HV: 48
-
CL: 874
Retrograde incremental pacing
-
Non decremental VA conduction
-
Midline activation
-
2:1 block

Antegrade incremental pacing
-
Broad complex tachycardia induced

12 lead ECG - tachycardia

Differential diagnosis
-
SVT with aberrancy
-
Antidromic AVRT
-
Ventricular tachycardia
Tachycardia characteristics
-
Long VA - 92ms

-
Tachycardia terminate with a V
VT unlikely diagnosis

Diagnostic maneouvres in tachycardia
-
HIS synchronous VPB showing atrial advancment

-
Ventricular entrainment
-entrains the atrium on <1 fully captured beats
VAV response

-
Ventricular entrainment
-PPI-TCL 404-314= 80ms
-Stim A - VA 150-80 = 70ms

-
Atrial entrainment
-pseudo AVVA response
-same QRS morphology
-VT excluded

-
All findings consistent with AVRT

Antidromic or orthodromic
-
HV 0ms during tachycardia (excludes aberrancy and consistent with antidromic AVRT)

Antidromic AVRT
-
HV interval 0ms during tachycardia
-
AVRT only tachycardia not ruled out
-
LBBB morphology
-
Retrograde conduction non-decremental (fixed VA)
-
Decremental antegrade pathway. AH prolongation seen with HV shortening with incremental atrial pacing
-
Pseudo AVVA interval with atrial entrainment pacing occurs due to antegrade decremental properties
-
However, all pacing maneouvres also showed a likely retrograde accessory pathway too.
-number of beats to entrain <1, +ve zipes
-
Antidromic and orthodromic AVRT?
-
To prove antridromic limb is part of circuit - assess with a lateral RA extra
Lateral RA extra
-
Advances next V without effecting immediate septal atrial activation

Mahaim Fibers
-
Atriofasicular pathway (RA connects to RBB fibers rather than RV)
-
Slow antegrade conduction via atriofasicular fibre with retrograde conduction via HIS bundle/AV node
-
Typically along the lateral tricuspid annulus
-
May be composed of AV node like tissue (decremental properties, adenosine sensitive)
-
Has a degree of automaticity & can spontaneously trigger AVRT
-
Minimal pre-excitation on ECG – often normal PR interval
-
LBBB appearance during AVRT or pre-excitation
-
Delivering an early A from the lateral wall advances or delays the ventricular signal, but the septal atrial electrogram is not advanced on the APB beat.

Mapping atriofasicular fibers

-
M potential during atrial pace
-
M potential during tachycardia

-
Morphology

-
Bump map with ablator

-
3D map - RAO


-
3D map - LAO


Post ablation testing
-
No evidence of pre-excitation
-
Decremental AV nodal properties shown
-
No inducible tachycardia
-
Confirmation that the tachycardia was antidromic AVRT using mahaim pathway is the antegrade limb and the AV node as the retrograde limb.
References
-
Alasti, M., Pawade, T., & Alison, J. (2022). Ventricular tachycardia or supraventricular tachycardia? Journal of Arrhythmia. 38; 259-262
-
Smeets, J.L.R.M, Hsia, H.H., Sanchex, J.M. et al (2019). Understanding the Mahaim pathway in the context of catheter ablation. Journal of innovations in cardiac rhythm management, 10 (1); 3509-3513