




Refractory rundown
-a clinical case on cardiac recovery-
Patient presentation
-
471 year old male
-
recurrent palpitations
-
multiple documented tachycardia on ILR
-sudden onset/offset
-narrow & broad complex
-regular (rates (~180ms)
-longest 10 minutes.



Differential diagnosis
-
AVNRT (+ with aberrancy)
-
orthodromic AVRT (+ with aberrancy or antidromic conduction)
-
Junctional tachycardia (+ with aberrancy)
-
Atrial tachycardia (+ with aberrancy)
Ventricular tachycardia and one of the options above
Baseline ECG/EGM
-
AH: 72
-
HV: 58


Retrograde incremental pacing
-
Midline retrograde atrial activation (earliest HIS A)
-
Decremental VA conduction
-
VA wenckebach at 335ms
Retrograde paced extras
-
MIdline (CS 9,10) decremental VA conduction
-
No retrograde jumps
-
VERP 260ms, VAERP <270ms

Antegrade incremental pacing
-
Decremental AV conduction
-
No evidence of pre-excitation
-
AV wenckebach 365ms

Antegrade incremental pacing



-
Occurs when the ERP of a distal site is longer than the FRP of a proximal site
-
When closely coupled stimuli are delayed enough at the proximal site to allow distal site recovery
-
Types
Gap phenomenon


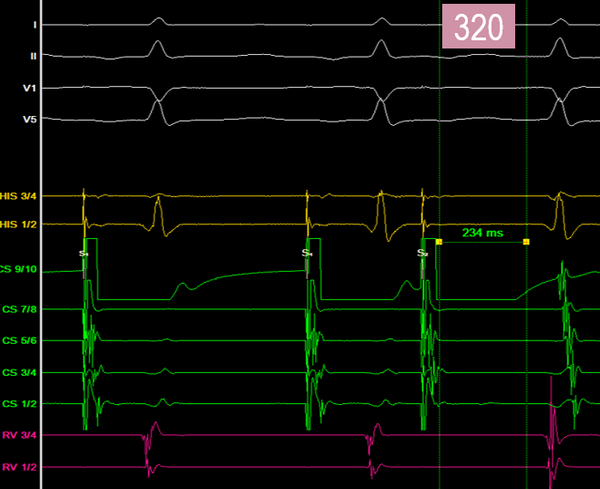
-
No evidence of pre-exictation
-
expected AH lengthening and jump with echoes 320ms
-
Atrial latency

-
Atrial ERP

-
•elay between the initiation of an electrical stimulus and the subsequent mechanical contraction of the atria
-
•acing latency, the time from atrial pacing to atrial contraction
-
Can be prolonged in certain conditions
-Hyperkelemia
-Myocardial disease
-Myocardial infarction
-antiarrhythmia drug toxicity
Atrial latency

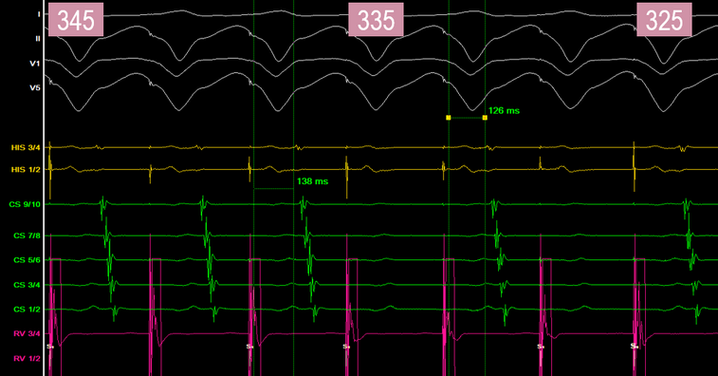
Tachycardia induction
-
Atrial paced doubles 1:1 with shortly became 2:1 (AVRT ruled out)
-
and then into a left bundle branch block - no change in VA interval also ruling out left sided pathway
-
midline atrial activation


-
May still be AVNRT with block from the slow pathway to the ventricle (lower common pathway block)
-
Also possible to have block from the fast pathway to the atrium (upper common pathway block) but is very rare
Lower common pathway block



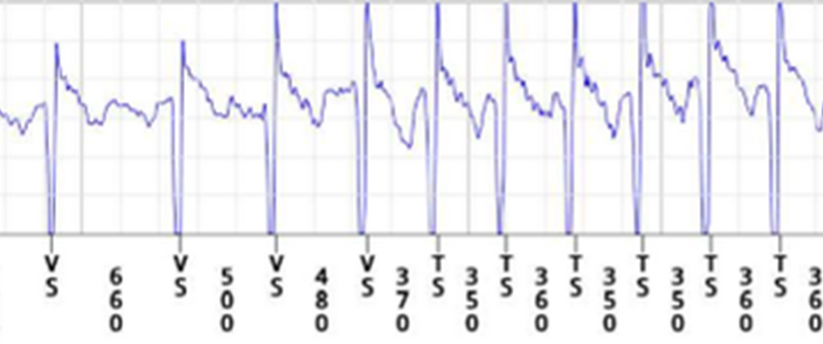
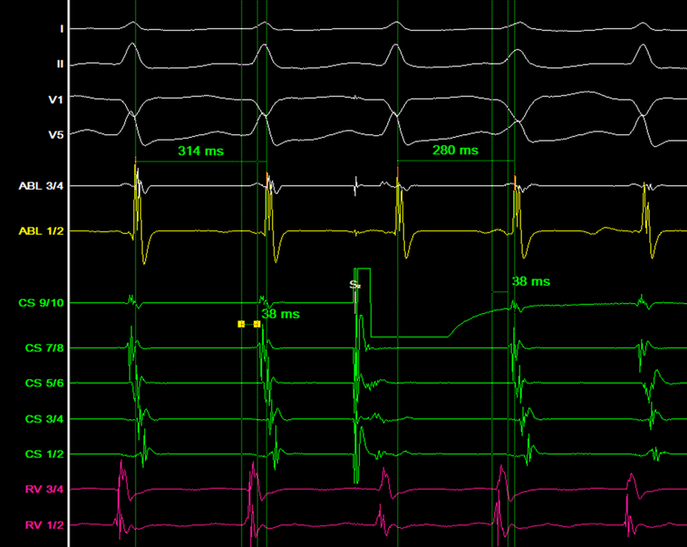
Ventricular entrainment -280ms
-
Ventricular entrainment performed which changed conduction back to narrow complex
-
V entrainment resulted in VAV response
-
>1 beat to entrain
-
PPI-TCL 150ms
-
Stim A - VA = 138ms

-
•The shortening of ERP due to an induced extra stimuli
Peeling back refractoriness

Late APB
-
Advances following HV (node part of antegrade circuit - JT effectively ruled out)
-
Same VA interval - node part of retrograde circuit (effectively ruling out ATc)
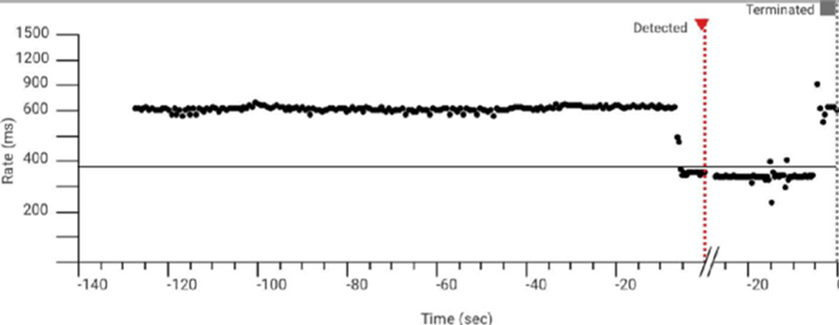
Tachycardia termination
-
Ends witt an A (Atc very unlikely)

Diagnosis

Slow pathway ablation performed
-
Good junctional rhythm seen during ablation.
-
No further tachycardia inducible post ablation.

References
-
Akrawinthawong, K. & Yamada, T. (2019). Typical atrioventricular nodal reentrant tachycardia with 2:1 conduction block: what is the mechanisms? Journal of arrhythmia, 21;35(2), 317-319
-
Cerna, L. et al., (2023). 1:1 Tachycardia initiated by a premature ventricular contraction: The curious appeal of the peel. Heart Rhythm Case Reports, Vol 9 (6), 391-395
-
Delon, W, Denes, P., Dhingra, R., & Rosen, K.M. (1974). Nature of the gap phenomenon in man. Circulation research, 34(5)
-
Klabundle, R.E. (2021). Cardiovascular physiolpogy concepts (3rd ed.).
-
Olshansky, B. & Sandesara, C.M. (2007). ECG 101: closing the gap phenomenon. EP Lab Digest
-
Tanabe, J., Fujita, S., Watanabe, N. & Tanabe, T. (2020). A case of prolonged atrial pacing latency. European heart journal, 4(4), 1-2