




VA-nishing act
-when fusion fails & confusion prevails-
Patient presentation
-
22 year old male
-
recurrent palpitations
-
documented tachycardia on ECG
-narrow complex, regular tachycardia
-long RP
-sudden offset

Differential diagnosis
-
AVNRT (atypical)
-
AVRT
-
Junctional tachycardia
-
Atrial tachycardia
Baseline ECG

Retrograde paced extras
-
MIdline (CS 9,10) non-decremental VA conduction
-
No retrograde jumps
-
VA ERP 380

Parahisian pacing
-
Same VA interval during RV only pacing and non-selective HIS capture
-
consistent with pathway conduction

Incremental atrial pacing
-
AV wenckebach 525ms
-
no evidence of pre-excitation

Paced atrial extras
-
No AH jump
-
AVN ERP 460ms

Sensed atrial doubles (on Isuprel)
-
Repeatable single echoes-
--Long VA (atypical echo)
-midline activation

Tachycardia induction
-
Induced with sensed atrial doubles on high dose Isuprel
-
Narrow complex tachycardia with midline atrial activation (CS 9,10)
-
TCL 318ms
-
VA interval 168ms

Tachycardia termination
-
Terminates with a V
-
Unlikely JT
-
Nothing else ruled out

HIS synchronous VPB
-
Shows atrial advancement
-active pathway (AVRT) or
-bystander pathway

HIS synchronous VPB
-
Shows tachycardia with VA block
-active pathway (AVRT)

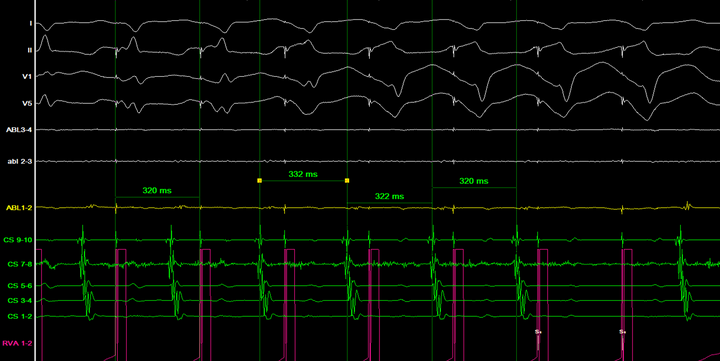
Ventricular entrainment - 320ms
-
Unable to entrain the atrium without terminating tachycardia
-
Entrains the atrium on the 1st fully captured beat
-consistent with AVRT
Diagnosis

Earliest activation
-
Postero-septal RA
-
Lack of VA fusion noted - quite separated VA



Post ablation
-
VA dissociation

Reasons for lack of fusion of VA at pathway insertion site
Slow conducting pathways (PJRT)
-
PJRT is a rare SVT (<1% of SVTs)
-
Rates vary between 120-250 bpm
-
Inverted p waves in II, III, aVF
-
PR interval shorter than RP interval
-
Usually near the ostium of the CS
-
May also have slow conduction if the pathway has been damaged (previously ablated with some recovery)

Oblique pathways
-
Oblique accessory pathways although rare, result in different location of the earliest atrial and ventricular activation sites.

References
-
Wang et al. (2015). An unusual atrioventricular accessory pathway with an oblique course. Heart rhythm case reports, 1(6), 411-415
-
Otomo, et al. (2001). Reversing the Direction of Paced Ventricular and Atrial Wavefronts Reveals an Oblique Course in Accessory AV Pathways and Improves Localization for Catheter Ablation. Circulation, 550-556
-
Parvin et al. (1999). Clinical Course of Persistent Junctional Reciprocating Tachycardia. Journal of the American College of Cardiology, 33 (2), 366-375
-
Dick (2010) Clinical cardiac electrophysiology in the young.