




Phantom bypass tract
-from pathway to runway-
Patient presentation
-
20 year old male
-
Aviation medical assessment
-12 lead ECG showing pre-excitation (not currently available) -
Asymptomatic
-
EP study to assess the pathway
-important to risk straitify the pathway for risk of SCD
-1.4% of WPW patients will have SCD
-EP assessment required to assess antegrade conduction >/=250ms
Baseline ECG/EGM
-
Normal AH and HV (70 and 40)
-
No evidence of pre-excitation

Retrograde incremental pacing
-
VA dissociation
-
No evidence of retrograde pathway conduction
Antegrade pacing
-
Dual AV node physiology
-
AV wenckebach 360ms
-
AH jump 340ms
-
AVN ERP 260ms
--(80ms tachycardia window)
-
No evidence of antegrade pathway conduction




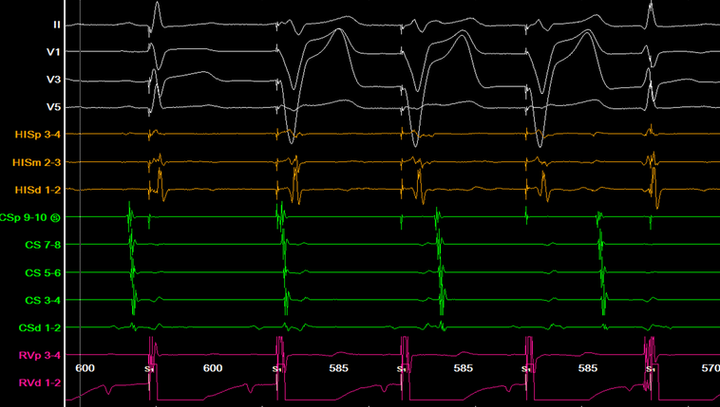
4mcg Isuprel infusion
Retrograde incremental pacing
-
Eccentric VA conduction (CS 1,2)
-
FIxed VA interval (non decremental)
-
Retrograde pathway ERP 350ms

Retrograde paced extras
-
Eccentric VA conduction on the extra (CS 1,2)
-
retrograde pathway ERP 270ms


Antegrade incremental pacing from CSd
-
Brief few beats seen with slight pre-excitation (HV 20ms)
-
Antegrade accessory pathway 390ms
-
Delta wave on time with CS 3,4

Atrial burst pacing
-
Repeatable atypical eccentric single echoes only

Ablation considerations
-
Symptomatic
-
Prognostic AP
-
Risk assessment
-transeptal
-proximity to AVN -
Need for occupation / dream job
Australian ablation recommendations
Class I
-
Symptomatic AVRT or
-
Pre-excited AF
Class IIa
-
Asymptomatic antegrade AP conduction </= 250ms or
-
Asymptomatic with pre-excitation which precludes specific employment
References
•Aleong, R.G., Singh, S.M., Levinson, J.R & Milan, D.J. (2009). Catecholamine challenge unmasking high-risk features in the Wolff-Parkinson-White syndrome. Europace
•Steinberg, C., Philippin, F., O’Hara, G. & Champagne, J. (2020). Orthodromic atrioventricular reentrant tachycardia using a concealed isoproterenol-sensitive accessory pathway.