top of page





-
Patient had dual chamber pacemaker (DDD 60-130) implanted for syncope and complete heart block
-
Presented with palpitations (ECG below)

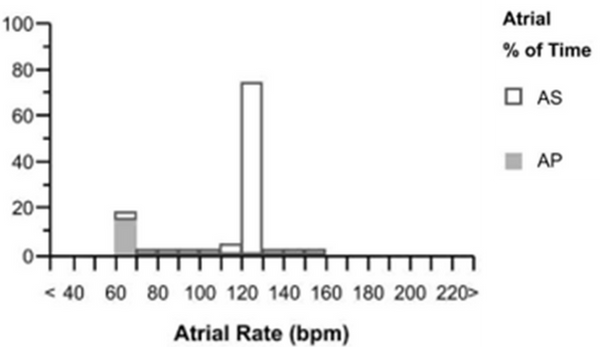
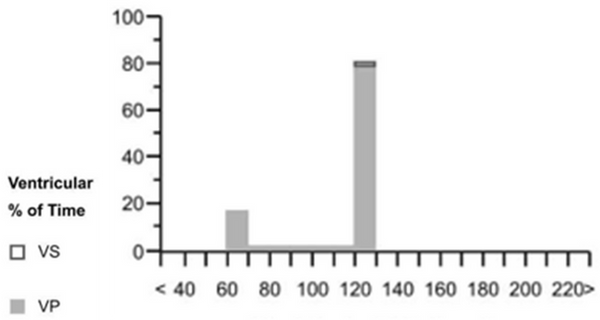
Small pacing spikes followed by a broad ventricular beat (ventricular capture) at ~120bpm
Intrinsic p waves prior to each QRS, appears to be tracked and is therefore sensed -DDD.
P wave morphology inverted in inferior leads. Inconsistent with sinus node origin.
Possible diagnosis: PMT or atrial arrhythmia
-
Arrhythmia was diagnosed as a PMT
-
PVARP was lengthened to avoid tracking retrogade As.
-
Search AV was turned off (not required due to CHB) which was triggerring PMTs
bottom of page