




-
88 year old female with dual chamber implanted for pause dependent VT
-
Currently programmed DDD 70-120
-
Underlying sinus rhythm


Reasons for pacing faster than base rate
Atrial fibrillation pacing algorithms
-
rate smoothing
-
AF suppression
-
post mode switch overdrive pacing
-
atrial preference pacing
-
Rate Response -
May only be on in a mode switch
-
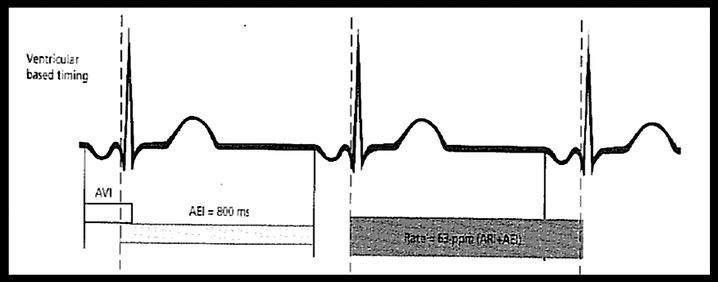
Ventricular based timing
-
Depends on the company and the mode
Atrial verse ventricular based timing
Atrial based timing
-
Pure: rate is driven by the LRI (AA interval)
-
-
Modified: rate is driven by the LRI (AA interval), except after VPB where VA timing is used
-
Ventricular sensed timing -
Rate is driven by VA interval (LRI - PAV interval)
-



Ventricular/ atrial based timing are non programmable
Shorten AV delays ?
-
this may result in higher/unnessary ventricular pacing
-
*Note: no search AV/VIP in DDI mode
Back to DDD with lower UTR ?
-
still may track noise
Decrease lower rate limit in DDI?
-
avoid pacing faster than necessary
Increase atrial sensitivity to a higher number and leave in DDD ?
-
may undersense true atrial events


