




Other device algorithms
ALL
•Mode switch – VVIR/DDIR]
(mode switching occurs to prevent ventricular tracking of fast atrial rhythms (AF/AFl/ATc) by temporarly changing the mode to a non tracking mode during episodes of fast atrial activity)
Biotronik (BTK)
•Rate stabilisation
•2:1 Lock in
Boston (BSC)
•Rate Smoothing
•Ventricular Rate regulation
Medtronic (MDT)
•Conducted AF response
•Ventricular Rate Stabilisation (VRS)
•Atrial Rate Stabilisation (ARS)
•Blanked flutter Response
Sorin
•Rate smoothing
Abbott
Auto mode switch (AMS)
●AMS begins when the intrinsic atrial rate exceeds the atrial tachycardia detect rate (ATDR) (programmable)
●A seperate base rate during an AMS episode can be programmed (AMS Base Rate)
●AMS ends when intrinsic atrial activity returns to a rate below the ATDR
●electrograms (EGMs) are stored for AMS episodes

●The algorithm distinguishes sustained tachycardia from intermittent fast cycles by calculating a Filtered Atrial Rate Interval (FARI), a value that compares the current rate to a running average rate.
●When the FARI exceeds the programmed ATDR value, the device stops tracking the atrial rate and switches to DDI(R) or VVI(R) mode.
●When the tachyarrhythmia subsides and the FARI falls below the Maximum Tracking Rate (MTR) or the sensor-indicated rate (whichever is faster), the device switches back to DDD(R) or VDD(R) operation.
●NOTE: During a mode switch, the programmed PVARP is replaced by the programmed setting of the Post Ventricular Atrial Blanking (PVAB). The lowest available PVAB period during a mode switch (and thus, the lowest PVARP) is 110 ms.

Accessed from Parameters; AT/AF detection and response
Auto Mode Switch: on, (DDI,DDIR, VVI, VVIR) off
AT/AF detection rate: 110 – 150 in steps of 5; 160 – 200 in steps of 10; 225 – 300 in steps of 25
AMS base rate: typically higher than the base rate (to avoid pt feeling sudden drops in HR). However, more RV pacing= increased AF, so a lower base rate may be preferable. (40-170 in steps of 5).


Biotronik
Mode switching
Onset criteria/resolution criterion: X of 8 (rolling counter) beats are faster than the MS rate to switch, or slower than the programmed rate to return to programmed base rate.

Accessed from
Mode Switching: on, off
Intervention Rate: 100-250 bpm (10 bpm increments) (160 bpm)
Switch to: DDIR
Onset Criteria: 3-8 (increments of 1) (5)
Resolution Criterion: 3-8 (increments of 1) (5)
Basic Rate during mode switching: off, +5- +30 (increments of 5) (+10)
Rate stabilisation during MS: on, off

Rate Stabilisation
to minimise sudden rate changes in the ventricle during MS. Uses rate fading: determines a four-beat ventricular rate average and provides ventricular support pacing any time the rate goes below the averaged rate -10bpm.
Accessed from
Mode Switching: on, off
Rate stabilisation during MS: on, off
2:1 Lock in
2:1 Lock in Protection: (similar to blanked atrial flutter) when senses 8 consecutive atrial events in the far-field window and the Vp response is >100 bpm, the AV delay is extended to a max value of 300ms for one event. If there is no variation in the A-A interval, the device will detremin ethe rhythm to be Aflu and MS.
Accessed from
Mode Switching: on, off
2:1 Lock in: on, off
Boston
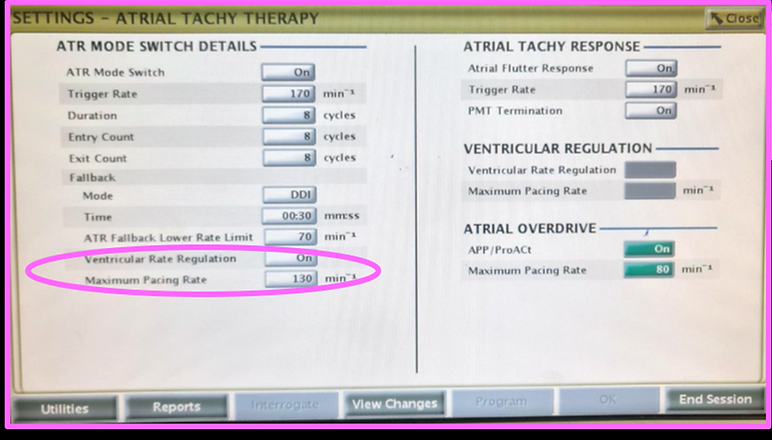
Atrial Tachy Response
Trigger Rate
The rate cutoff at which the pacemaker begins to detect AT.
Duration
Determines the number of ventricular cycles during which the atrial events continue to be evaluated after initial
detection. If the AT persists for the programmed duration, mode switching occurs and the ventricular rate decrease to
the sensor rate or the ATR lower rate limit.
Entry Count
Determines how quickly an AT is initially detected. Once the number of fast atrial events detected equals the programmable Entry count.
Exit Count
Determines how quickly the AT response algorithm is terminated once the atrial arrhythmia no longer is detected.
Fallback Mode
Once duration has been fulfilled, the pacemaker will automatically switch to the programmed fallback mode.
Fallback Time
Determines how quickly the rate in fallback will decrease to the ATR lower rate limit or sensor rate. The fallback time controls the decrease in the paced rate. During fallback rate smoothing, rate hysteresis and search hysteresis are disabled. When the pacemaker is permanently programmed to an adaptive rate mode with an adaptive rate ATR fallback mode, the pacemaker will use the sensor and sensor parameters already in effect at the time of the switch.
Lower rate limit
The ATR lower rate limit allows an independently programmed lower rate during mode switch

Accessed from Brady Parameters; A-Tachy Response
Trigger Rate: 100-200 bpm (5 bpm increments) (170 bpm)
Duration: 0, 8-2048 cycles (powers of 2) (8 cycles)
Entry Count: 1-8 cycles (increments of 1) (8 cycles)
Exit Count: 1-8 cycles (increments of 1) (8 cycles)
Fallback Mode: VDI (R), DDI(R)
Fallback Time: 0-120 seconds (5 second increments) (30 seconds)
Lower Rate Limit: 30-50 bpm (5 bpm increments), 50-90 bpm (1 bpm increments), 90-150 bpm (5 bpm increments) (70 bpm)

Rate smoothing
•Rate Smoothing is a programmable feature that controls the pacemakers response to atrial and/or ventricular rate fluctuations that cause sudden changes in pacing intervals.
•This feature is beneficial predominantly for patients with SSS, PACs, PVCs, PPM wenckebach, brief SVTs/AF/AFl, and retrograde p-waves.
•Pacemaker patients who experience large variations in their ventricular paced rate can feel symptomatic during these episodes. Rate smoothing can prevent these sudden rate changes and their accompanying patient symptoms (such as palpitations, SOB, and dizziness).
•Rate smoothing can significantly reduce rate fluctuations associated with the onset and cessation of atrial arrhythmias.
•Rate smoothing operates between the lower rate and the max track rate or sensor rate (whichever is highest) in non-adaptive rate modes.
•When programmed on rate smoothing values are a percentage of the R-R interval.
•The rate smoothing up parameter controls the largest increase allowed in the pacing rate when the intrinsic or sensor rate is increasing.
•The rate smoothing down parameter controls the largest decrease allowed in the pacing rate when the intrinsic or sensor rate interval is decreasing.
•Rate smoothing is functional except when search hysteresis is in action, during ATR fallback, and PMT termination. Rate smoothing cannot be programmed on when sudden brady response is on.

Accessed from brady parameters; rate enhancements
Rate Smoothing Up: off, 3-24% (3% increments)
Rate Smoothing Down: off, 3-24% (3% increments)



Atrial flutter response
Works similarly to the Medtronic blanked flutter search, to avoid tracking blanked flutter.


Ventricular rate regulation
•Designed to reduce V-V cycle length variability during conducted atrial arrhythmias.
•The VRR algorithm calculates a VRR indicated pacing interval based on a weighted sum of the current V-V cycle length and the previous VRR-indicated pacing intervals (this is similar to rate smoothing, which only uses the most recent V-V interval however).
•When programmed on in tracking modes, VRR is active only when an ATR mode switch has occurred.
•Once tracking mode operation resumes at the termination of the atrial arrhythmia, VRR becomes inactive.
•In SR modes, VRR is continually active. When rate smoothing is turned on with VRR, rate smoothing is disabled during MS.
•VRR Max Pacing Rate: limits the maximum pacing rate the VRR algorithm can reach.
Accessed from Brady Parameters; A-Tachy Response
Ventricular Rate Regulation: off, on (DR: on; SR: off)
VRR Max Pacing Rate: 60-150 bpm (5bpm increments) (110 bpm)


Medtronic
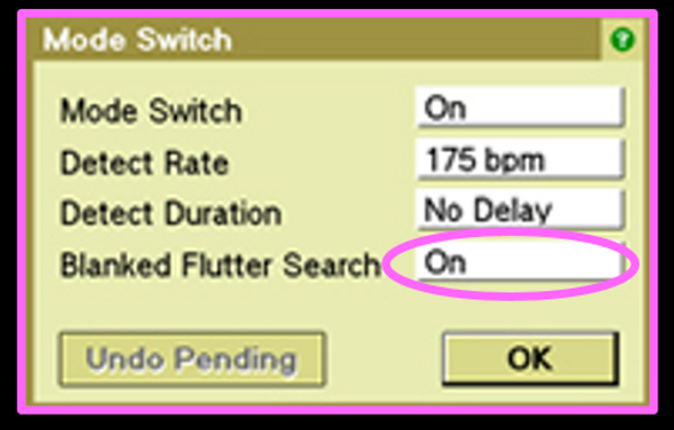
Mode Switch
Whenever any 4 of the previous 7 A-A intervals exceed the programmable Mode Switch detection rate for the duration of the detect duration delay, the pacemaker will Mode Switch to DDIR.
The ventricular rate is gradually decreased and the mode switches to DDIR.
When either 7 A-A intervals are < than the UTRi, rate drops below detect rate or 5 AP occur the ventricular rate is gradually increased and the mode switches back to DDDR.

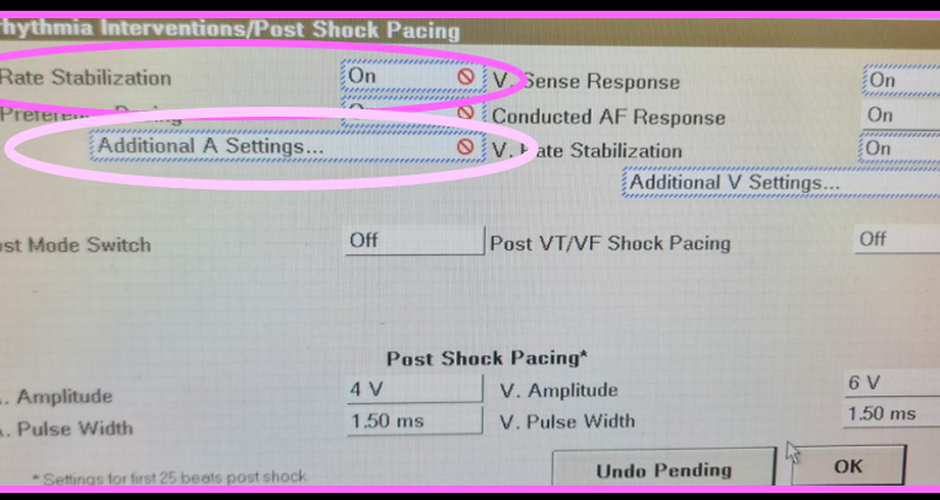
Conducted AF response
•intended to regularize V-V intervals in patients with an irregular ventricular response during AF. Conducted AF Response modifies the pacing rate on a beat-by-beat basis to pace at, or just above, the mean intrinsic rate
•increases the percent of ventricular pacing without significantly raising the average pacing rate (useful for biventricular devices)



Ventricular Rate Stabilisation
•When a patient experiences a PVC, it is often followed by a long pause in the cardiac cycle. This pause is sometimes associated with the onset of pause-dependent ventricular tachyarrhythmias.
•Ventricular Rate Stabilization (VRS) is a programmable feature designed to eliminate the long pause that commonly follows a PVC.
•VRS responds to a PVC by increasing the pacing rate, then gradually slowing it back to the programmed pacing rate or intrinsic rate.
•VRS cannot work simultaneously with CAFR. Both can be programmed on together, but when this happens, CAFR will occur during AMS, and VRS will occur during normal DDD mode.
•When VRS is enabled, it acts as a constant rate-smoothing algorithm by adjusting the ventricular intervals that may follow a PVC.
•Following each successive ventricular sense or ventricular pace event, the device calculates a new pacing interval by adding the programmed interval increment value to the previous pacing interval.
•The calculated interval lengthens, from beat to beat, until the device returns to the intrinsic rate or the programmed pacing rate, whichever occurs first.
•The pacing rate increase determined by VRS, however, does not exceed the maximum rate programmed for this feature.
•On each PVC, the device calculates a new ventricular interval as:
New R-R interval
= previous R-R interval + programmed Interval Increment value
(or a predetermined minimum interval* if it is larger than this sum)
Accessed from parameters; pacing; arrhythmia interventions; V rate stabilization
V Rate Stabilisation: on off
Maximum Rate: 120
Interval Increment: 150 ms




Atrial Rate Stabilisation
•Atrial Rate Stabilization (ARS) is a programmable feature designed to prevent the long sinus pause that commonly follows a premature atrial contraction (PAC).
•When ARS is enabled, at each atrial event (AS event, AP event, or pertinent AR event*), the device calculates a new pacing interval, which is equal to the current pacing interval increased by the Interval Percentage Increment.
•If the current pacing interval ends before the device senses an atrial event, the device delivers an atrial pace and recalculates its interval using the current atrial interval.
•The current pacing interval will be the shorter of the sensor rate interval or the calculated interval.
•The programmed Maximum Rate value provides a rate limit for operation of the feature.
•After a PAC, the calculated escape interval stabilizes the atrial rate and gradually slows it to the intrinsic rate, sensor-indicated rate, or programmed Lower Rate (whichever is attained first).
The following diagram illustrates ARS operation. ARS pacing begins when a premature beat occurs, and ends when the sensor rate or lower rate is reached.

1.Pacing occurs at the programmed escape interval.
2.The premature beat initiates a shorter escape interval. This interval ends with a programmed pace, which is determined by the maximum rate.
3.The device uses this atrial interval to calculate the next escape level.
4.This atrial interval is 25% longer than the preceding one. It ends with the second programmed pace.
5.When the calculated pacing interval exceeds the programmed escape interval, normal pacing resumes.


Blanked Flutter Response
•Functions to unveil possibility of blanked flutter
•Device looks at 8 consecutive intervals where the AA <TARP and <2x USR
•Extends PVARP on 9th interval (similar to PMT intervention algorithms) to uncover is there a 2nd As that would otherwise be hiding in post ventricular atrial blanking period

Microport
Rate smoothing
The Smoothing function is designed to prevent a sharp rate drop to the programmed basic rate in patients presenting with episodes of paroxysmal bradycardia.
•If the patient’s spontaneous rate drops, the pacemaker takes over at a rate slightly lower than the spontaneous rate immediately prior to the pause.
•The pacing rate is then gradually reduced until the basic rate is reached or the spontaneous rhythm is restored.
