




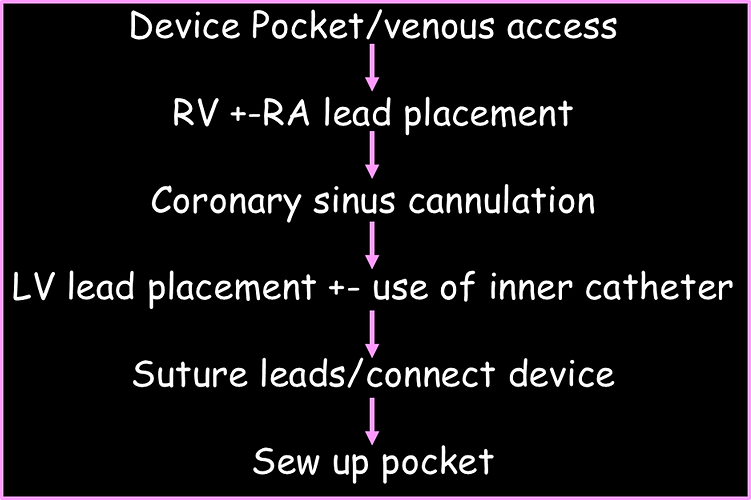
Transvenous CRT implant

Equipment

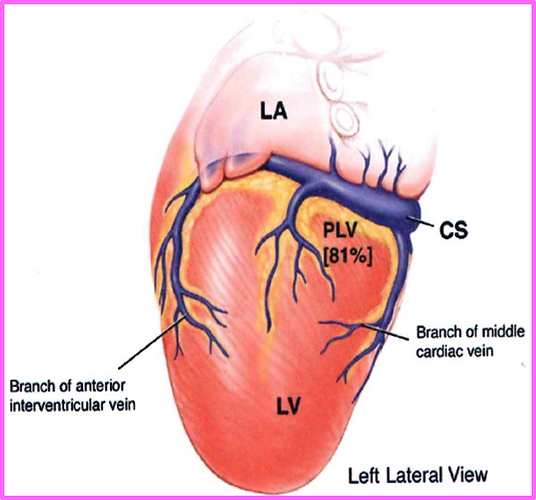
CS anatomy & physiology
Returns deoxygenated blood to the right atrium from the epicardial ventricular veins
•Oxygenated blood circulates to the coronary arteries to supply the ventricles prior to circulating back to RA
Epicardial ventricular veins include
•The great cardiac vein – anterior
•The middle cardiac vein – posterior
•The small cardiac vein – RV
•The veins of the LV
•Posterior
•Lateral


Coronary Sinus Cannulation
Different shaped curved sheaths for cannulation
•Shape determined by Dr preference, RA size & CS anatomy
The ideal curve allows the body of the catheter to rest against the free wall of the RA and engage the CS os, allowing stability and torque application to probe the ostial septum anterior to the Eustachian ridge in both the anterio-posterior and supero-inferior directions.
Difficulty engaging the CS
•CS os and course of CS are not in expected fluoroscopic planes
•Large RA
•Prominent thebesian valve
•Abnormalities of the CS (e.g., stenosis, torturosity, congenital)
•Complete occlusion of CS
Cannulating the CS is typically performed with fluoroscopy and contrast injections.
Balloon tipped catheter can be used to assist visualising CS
•Balloon inflated just after the injection to stop the backflow of the contrast out of the CS.
•The fat pad can also be used to help visualise where the CS is
After CS cannulation an inner catheter may be used to help
