




Biventricular algorithms
Summary
Abbott
Negative AV hysteresis
Automatically shortens PAV/SAV when a VS occurs.

Autovect Select
Accessed from Parameters; CRT tool kit; perform autovect select
Assesses V-V delays with RV only pacing, LV only pacing and with intrinsic rhythm.
Determines differences in timing on each LV vector (for IS4 leads).
Recommends most optimal pole/vector to pace from.



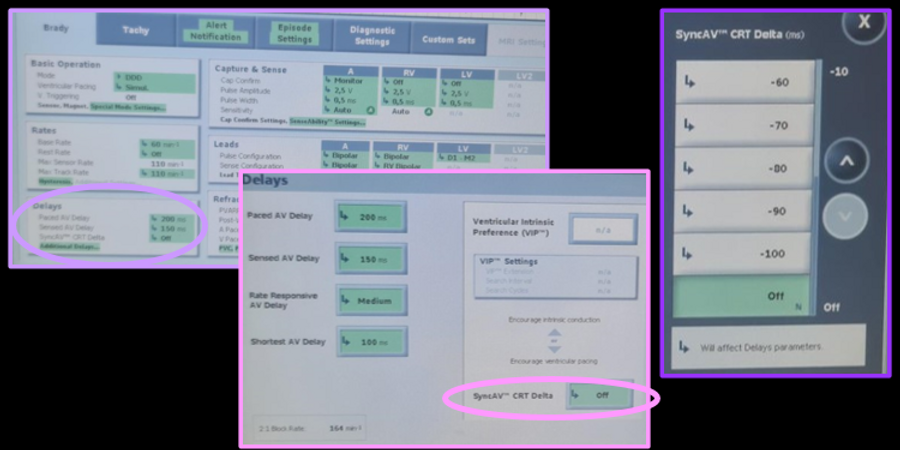
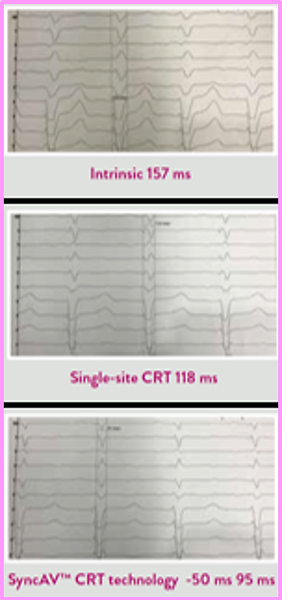
Sync AV
Accessed from Parameters; CRT tool kit; perform syncAV
For patients with
•intact AV conduction with AV delays <300ms
•LBBB
•sinus rhythm (not AF/low AF burden)
•low/no VPB burden
Sync AV works by
•Every 256 cycles the AV delay is set to the programmed value for 3 cycles (in this example 225 ms)
•AV conduction occurs intrinsically and SyncAV™ CRT technology measures the conduction time
•SyncAV™ CRT technology adjusts the AV delay for the next 256 cycles using the following equation: AVD = (Intrinsic Conduction Time) – (SyncAV™ CRT technology Delta
Abbott recommendations for programming
•After -50 ms, go to -60 ms then to -40 ms and evaluate QRS duration versus -50 ms to determine directionality.
•Then step up or step down in 10 ms increments to find the narrowest QRS
Note: When programming SyncAV™ CRT technology ON, Rate-Responsive AV Delay (RRAVD) is automatically turned OFF. This should remain OFF and can be found on the Delays screen
Warning: If on a conduction search there is no AV conduction, it defaults to programmed AV delay (likely to be suboptimal (too long))





Sync AV Plus
Accessed from Parameters; CRT tool kit; perform sync AV plus
ONLY AVAILABLE IN GALLANT & NUTRINA
For patients with
•intact AV conduction with AV delays <300ms
•LBBB
•sinus rhythm (not AF/low AF burden)
•low/no VPB burden
Sync AV PLUS works by
•Every 256 cycles the AV delay is set to 350 ms for AP-VS and 325 ms for AS-VS
•Intrinsic AV Conduction occurs and SyncAV™ Plus CRT technology measures the conduction time
•SyncAV Plus CRT technology adjusts the Paced and Sensed AV Delays for the next 256 cycles using the following equation:
AVD = (Intrinsic Conduction Time for AP or AS) – (SyncAV Plus CRT technology Delta)
In SyncAV Plus CRT, the calculated AV delays are based on RA to RV conduction times. For LV-first pacing, the VV delay is then subtracted from each calculated AV delay.
Abbott recommendations for programming
•After -15% (or -50 ms), go to -20% (or -60 ms) then to -10% (or -40 ms) and evaluate QRS duration versus 15% (or -50 ms) to determine directionality.
•Then step up or step down in 5% (or 10 ms) increments to find the narrowest QRS.
Note: When programming SyncAV™ CRT technology ON, Rate-Responsive AV Delay (RRAVD) is automatically turned OFF. This should remain OFF and can be found on the Delays screen





QuickOpt
QuickOpt measurements can be used as a one off recommendation for VV and AV programming recommendations.


Biotronik
Negative AV hysteresis
AV delay is shortened when a sensed beat occurs
It is shortened for 180 cycles before reverting back to initial programming


Trigerring
When a RV sense occurs, LV pacing will occur (VVT)
Max trigger rate can be programmed


LV T wave protection
Designed to prevent LV pacing in the vulnerable period
Inhibits LV pace when LV sense occurs
May unintentionally minimise BiV pacing percentage due to LV pace inhibition
ot Our Start


Auto LV VectorOpt
Involves assessment of RV-LV timing and the option of performing automatic threshold testing on all/multiple LV vectors.
RV-LV conduction time can be assessed by selecting the LV VectorOpt tab under tests, selecting RV-LV cond. time and selecting measure.
LV thresholds can be performed under the LV VectorOpt tab by selecting Auto, ticking the desired vectors to be tested and selecting start



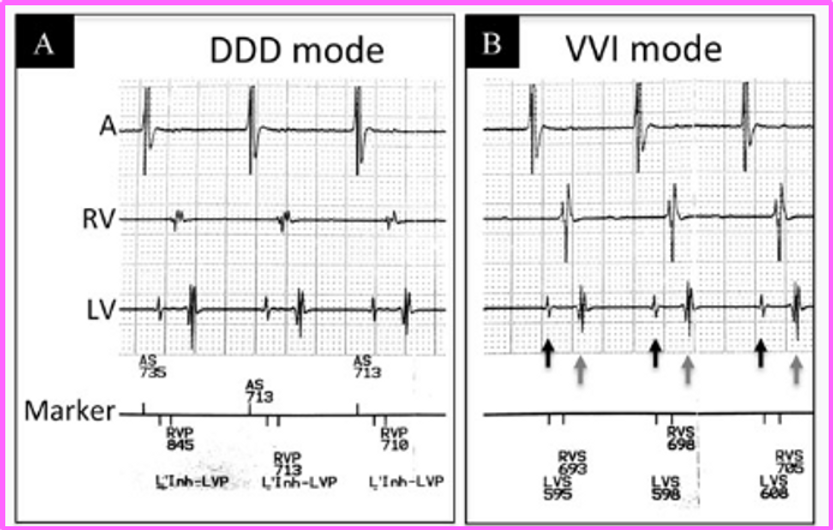
CRT AutoAdapt
Can automatically adjust AV delay and can set the ventricular pacing to BiV or LV only.
For this to occur
-must be in sinus rhythm
-rate <100 bpm
-A-RV conduction time after pace <250ms
Algorithm operation
-intrinsic conduction is assessed every 1 minute where the AV interval is extended to 300ms. If there is any AV block, the test interval is doubled up to 17 hours.
-If A-RV < A-LV timing (LBBB pattern), LV only pacing is utilisied
-If A-RV =/> A-LV BiV pacing is utilised
Programming
-Parameters; Ventricular pacing; CRT AutoAdapt
-On - for AV and BiV/LV adaptive pacing (LV autocapture must be on); or
AVadapt - for AV adjustments only



Boston Scientific
SmartCRT
SmartCRT includes
-Vector guide
-Smart delay
-Multisite Pacing
Vector guide - choose optimal vector
-performs auto thresholds along all LV vectors, compares impedance values and looks at RV pace - LV sense times
-phrenic stimulation can also be entered
-can be found under Tests; LV vector guide

Smart delay
-automated tests to recommend the following parameters
•sensed AV delay
•paced AV delay
•ventricular pacing chamber (biV or LV-only)
-is only performed at an in visit check (not continually updated)
-can be found under Parameters; normal brady/CRT, SmartDelay optimization


Multisite Pacing
-allows the option of selecting 2 LV vectors and offsets
-SmartVector automatically recommends vectors with 1-click
-SmartOffset automatically recommends offsets with 1-click
-can be accessed under parameters; settings - normal brady/CRT; LV multisite pacing

Triggered pacing
Biventricular paces when a RV sensed beat occurs
Limited by what the max pacing rate is set to
Counted towards the RVs & LVp counters
•E.,g 70% RV pacing, 100% LV pacing really equals
•70% BiV pacing with 30% biventricular fusion pacing
If device is programmed to RV only or LV only pace, and biv trigger pacing is ON, pacing in both chambers will still occur with triggered pacing


LV protection period
Designed to prevent LV pacing in the vulnerable period
Inhibits LV pace when LV sense occurs
Inhibits schedules LV pace from 300-500ms

Tracking Preference
Helps increase biventricular pacing/ventricular tracking when Atrial sensed beats are falling into PVARP.
When 2 consecutive AS fall into PVARP, PVARP is shortened until tracking occurs
Must be within the UTR limits

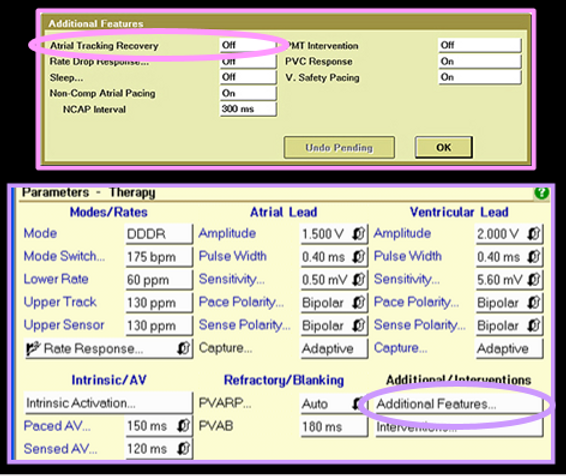
Medtronic
Atrial tracking recovery
Monitors for sustained episodes (8 beats) of VS slower than the UTR, due to atrial activity falling into PVARP. (poor programming (TARP too long)– not allowing for appropriate 1:1 pacing at upper rates – upper rate behavior)
PVARP temporarily shortened to allow for appropriate tracking

V sense response
Essentially allows the device to function in a ventricular tracking mode (e.g., VVT or DDT)
When a VS event is detected a VP is immediately triggered
Only potentially useful in patients with true AV conducted beats.
Ineffective on VPBs and may be proarrhythmic (no use for dependent patients)


Conducted AF response
Can increase the pacing rate during a mode switch episode or single chamber modes (VVI/VVIR) to account for faster ventricular rates in AF
Dynamically adjusts the rate up or down depending on the previous response
•VS adjusts the rate up (max 3 bpm at a time)
•VP adjusts the rate down (1 bpm at a time)


Adaptive biventricular pacing
On top of the option of adaptive BiV and LV pacing with LV only pacing, this algorithm has the ability to adjust AV and VV delays without compromising significant ventricular pacing.
Operation
•Every 1 minute an intrinsic AV delay is assessed (AV delay to 300ms)
•If no AV conduction, the search extends out by doubling (2min, 4min… max 16hrs)
•Every 16 hours the p wave width and QRS width is assessed
•The AV delay is updated based on intrinsic AV interval and P wave width
•The AV delay is adjusted to paced 30ms after the p wave but at least 50ms prior to the intrinsic QRS (provides enough atrial contraction time)
•VV delay is adjusted every 1 minute based on intrinsic RV to LV delay
Conditions
•Depending on model intrinsic AV delay
must be SAV<200/220 and PAV <250/270
•Suspended during tachyarrhythmias

Microport
The SonR sensor consists of a micro-accelerometer embedded in the tip of the SonRti atrial lead.
SonR measures the vibrations generated by the myocardium during cardiac contractions, which are correlated to LV dP/dt max.
The SonR sensor continuously measures the contractility of the heart allowing for automatic optimization of AV and VV intervals.
Optimization is performed on a weekly basis both at rest and during exercise. This allows for cardiac resynchronisation therapy to be continuously adapted to the individual needs of each patient
SonR signal measurements
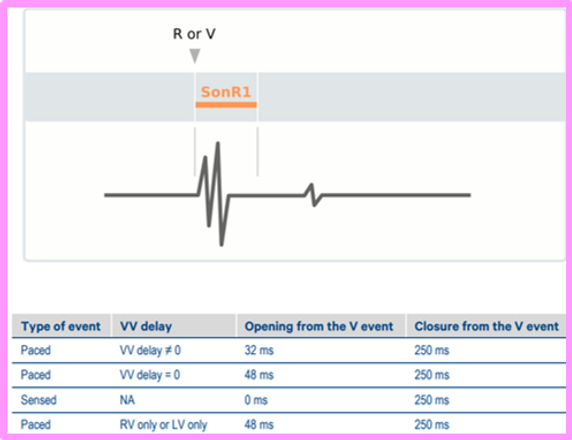
•measured as the Peak-to-Peak amplitude of the SonR1 component
•performed inside one window which is opened on a paced or sensed ventricular event
•the opening of the window from the ventricular event depends:
- on the VV delay applied: if it is not 0 ms, the window opens on the second event
- on whether the ventricular event is paced or sensed
Manual mode
•used during an in-clinic follow-up, the optimization is launched through the programmer and the device will provide optimal VV and AV delays at rest
Automatic mode
•when programmed on “AV+VV”, the algorithm calculates the optimal VV delay at rest and AV delays at rest and at exercise on a weekly basis in between follow-ups.
•the first optimization starts at midnight of the same day, then every Monday at midnight.
VV and AV Delays optimisation steps
1. VV delay optimisation at rest
2. AV delay optimisation at rest
3. AV delay optimisation at exercise
Rest conditions
• pacing rate based on the rate response sensor ≤ Basic rate + 5 bpm (only if rate response is programmed),
• heart rate < 90 bpm over 8 atrial cycles (in automatic modeb )
• no ventricular or atrial premature contractions (PVCs or PACs)
• no tachyarrhythmia detection
VV delay optimisation at rest
• The device will test VV delays at 6 predetermined AV delays (refer to Microport academy for complete details)
• 7 fixed VV configurations with these 6 AV delays are then tested to calculate the average amplitude of the SonR signal
(LV-RV 48ms, LV-RV 32ms, LV-RV 16ms, BiV sim, RV-LV 16ms, RV-LV32ms, RV-LV 48ms).
• A contractility index for each VV delay configuration will then be calculated based on the area under the curves from the average amplitude of the for the different VV and AV delay combinations SonR signal


AV delay optimisation at rest
• only starts once optimal VV delay is determined
• occurs at 1am for sensed AV
• occurs at 2am for paced AV
• AV delay extended to 300ms
• base rate -10ms hysteresis to average ventricular rate for sensed AV and +10ms to a sensed rhythm for paced AV
• calulates as average of 8 beats to a maximum of sensed AV 224ms and paced AV 264ms.
• Tests 11 different AV delay settings with the shortest at 32ms up to the maximum value
• The optimum AV delay is then chosen from the middle of the plateau of the 3 segment sigmoid curve

AV delay optimisation at exercise
• the trigger for the AV delay optimisation is the patients heart rate
• once this value is his (programmable - nominal 90), optimisation begins
• only 5 different AV delays are tested
-2 AVD shorter than the last optimal AVD at exercise
-2 AVD longer than the last optimal AVD at exercise
• the length of the intervals will depend on the patient’s PR/AR interval at rest
-If the (PR/AR at rest – 47ms) > 96 ms, the AVD will be calculated in steps of 16 ms.
-In case the (PR/AR at rest – 47ms) < 96 ms, the AVD will be calculated in steps of 8 ms

Programming SonR

Evaluating SonR CRT Optimisation test results
The histograms of the mean SonR signal values (measured immediately after spontaneous or paced beats, or PVCs) are displayed in blue at the bottom of the screen week after week, and can be used to assess its trend over time and to gauge the evolution of cardiac function. The cursor allows moving from one week to another and to clearly view on the right side of the screen, the VV interval and applied sensed AV delay (implied, after sensed P wave), and paced AV delay (implied, after paced P-wave) values as well as the mean SonR amplitude measured during the week. The choice of AV delay curves is obtained by clicking on the « Rest » and « Exercise » buttons under the « Activity » heading, and on « Sensed » and « Paced » under the « Rhythm » heading.

Optimisation Test
